Researchers at the Department of Paediatrics, Emma Children’s Hospital, Amsterdam UMC and University of Amsterdam, The Netherlands, have reported a research study on the phenotype, genotype, biochemistry and treatment effects of GACR, potentially valuable to be used for care pathways and clinical trial design. The study describes “the largest cohort of molecularly diagnosed individuals with gyrate atrophy of the choroid and retina (GACR) reported in the last 20 years” and provides “insights into effects of current therapies and extends knowledge on biochemical abnormalities in the disease”.
GACR is a rare inherited metabolic disorder characterized by progressive loss of vision, often begin in early childhood with night blindness and constriction of the visual field (VF), due to progressive chorioretinal degeneration. Patients receive a marked central vision loss and legal blindness when the macula may become affected and many patients have high myopia and develop early cataract and cystoid maculopathy. The disorder arises from biallelic pathogenic variants in OAT – the gene encoding mitochondrial matrix enzyme ornithine-δ- aminotransferase (OAT). Profound hyperornithinemia can cause from excessive ammonia accumulation, and can develop secondary creatine deficiency in brain and muscle tissues. Essentially, ornithine is the toxic agent and a reduction in plasma ornithine might slow disease progression however, there is not curative treatment. A natural protein-restricted (arginine-restricted) diet may support GACR patients but severe visual impairment may persist.
In their study, 27 patients were evaluated that showed a significant association between dietary natural protein intake and plasma ornithine levels and ornithine increased significantly with age, independent of dietary natural protein intake. There was no statistically significant association between ornithine levels and best-corrected visual acuity (BCVA) over time. In their paper, the researchers reported that 12 of 27 patients had a decrease in plasma ornithine (µmol/L) after initiation of therapy; 5 of 27 patients had stable plasma ornithine values and 10 of 27 patients had increased plasma ornithine, despite ornithine-lowering strategies (see figure below, coloured regression lines showing ascending, descending or stable for the 27 patients):
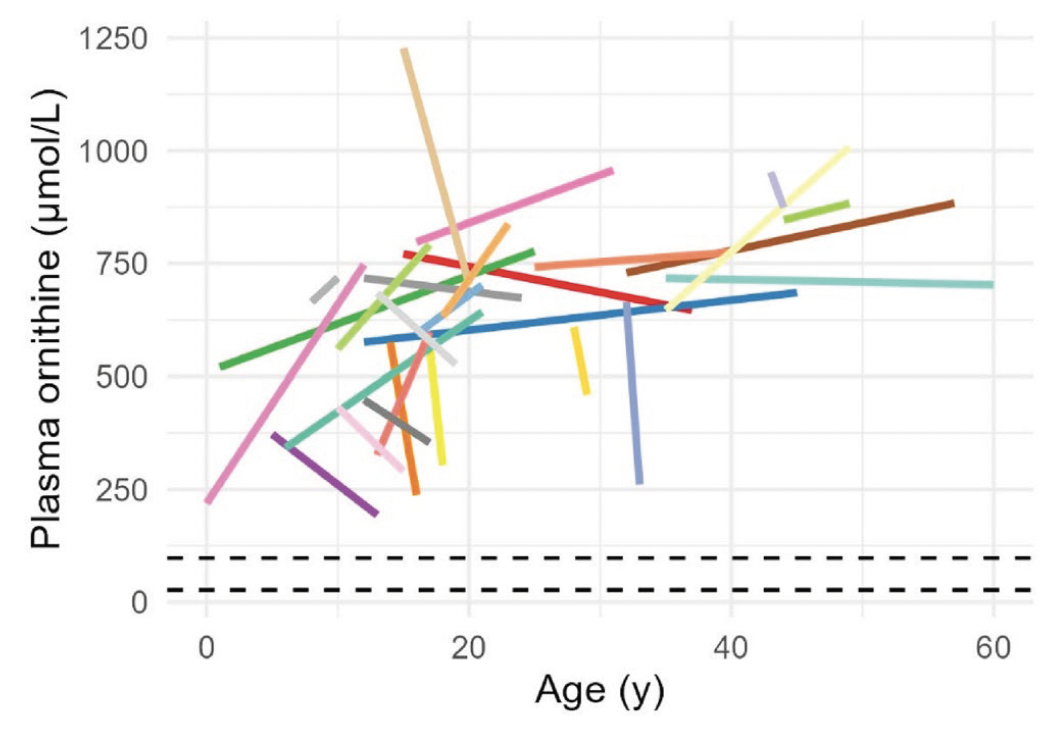
Figure 1: Plasma ornithine over time in patients with GACR with and without therapy. Different colours indicate different patients. Linear regression was used to draw regression lines for each individual patient. The dashed lines delineate the reference range for plasma ornithine in our reference laboratory (27 and 98 μmol/L). A scatterplot with individually plotted ornithine values can be found in their supplemental information. [Open access article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format when proided to the appropriate credit of: Balfoort et al, J Inherit Metab Dis. 2025 Jan 6;48(1):e12842. doi: 10.1002/jimd.12842].
The researchers also reported that patients who started a natural protein-restricted diet below 10 years of age had better VF outcomes, compared to patients that started at a later age. A notable finding was the presence of early bilateral cataract, high myopia, and severe constriction of VF, which showed that 44% of patients (n = 12) had undergone cataract surgery and the mean age at cataract surgery was 28 years (SD 1.9, range 18–37.5). In their summary, the Dutch researchers commented that, “a natural protein-restricted diet might help in slowing down disease progression if started early in life. GACR requires a multidisciplinary management approach including the following health care providers. A thorough knowledge of the phenotype and clinical course, preferably in prospective multicentre clinical studies, will a steppingstone toward the development of novel clinical endpoints for future clinical treatment trials to improve patient outcomes and quality of life”.