Researchers at UCL Institute of Ophthalmology, University College London, and Moorfields Eye Hospital NHS Foundation Trust, UK, have reported a study on CNG3A-associated achromatopsia (ACMH), a disorder which is targeted in several gene therapy trials over recent years. Given that the disorder provides a relatively intact foveal retinal structure, it is an attractive gene therapy candidate with a stable pathology and a large potential treatment window. According to the researchers, adaptive optics scanning light ophthalmoscopy (AOSLO) has allowed “the characterization of the foveal cone mosaic in ACHM by identifying individual cone photoreceptors in both CNGB3 and CNGA3 genotypes, as well as the rarer genotypes of ATF6, GNAT2”. Evaluating cone photoreceptors in vivo “may prove to be a useful tool for defining the therapeutic benefit of candidate treatments and potentially stratifying patients by treatment prognosis using foveal mosaic metrics to better inform patient selection for clinical trials”.
Researchers commented that there is a limited body of literature on CNGA3-ACHM imaging with AOSLO, and with no longitudinal studies reported to date. Achromatopsia is a rare autosomal recessive inherited retinal disorder (IRD) with an estimated prevalence of 1:30,000 to 40,000, characterized by reduced central visual acuity (<20/200), pendular nystagmus, photophobia, eccentric fixation and reduced or complete lack of colour discrimination. The disorder is an autosomal recessive condition caused by mutations in one of six genes: CNGB3, CNGA3, GNAT2, PDE6C, PDE6H and ATF6. CNGA3 and CNGB3 (the cone-specification channel cyclic nucleotide gated channel α and β3) are estimated to account 75-80% of all cases. The diagnosis is generally made on electrophysiology (ERG) where cone cell function is absent, while in contrast, rod function is normal. The disease is essentially stable. The glare and photophobia can be ameliorated with either a brown or red tint in glasses and currently there is no treatment.
In their current study, the UK researchers reported a mean (±SD) age 27 ± 10.3 years (at the first visit) with a CNGA3-ACMH diagnosis, with a follow-up of 2.6 ± 1 years. Their results showed no change in ONL thickness, degree of EZ disruption, or foveal hypoplasia over the follow-up period and observed a stable foveal cone mosaic using AOSLO imaging, with no significant change in peak cone density (PCD) and inter-cell distance (ICD). The mean PCD was 15,346 cones/mm² at the mean age of 29 years old (cf. 64,000–324,000 cones/mm² in previously reported healthy controls), with a mean rate of change of –117.79 cones/mm² (0.8%) per year, P = 0.130. The mean ICD at the mean age was 13.82 µm, with a rate of change of 0.17 µm per year, P = 0.83.
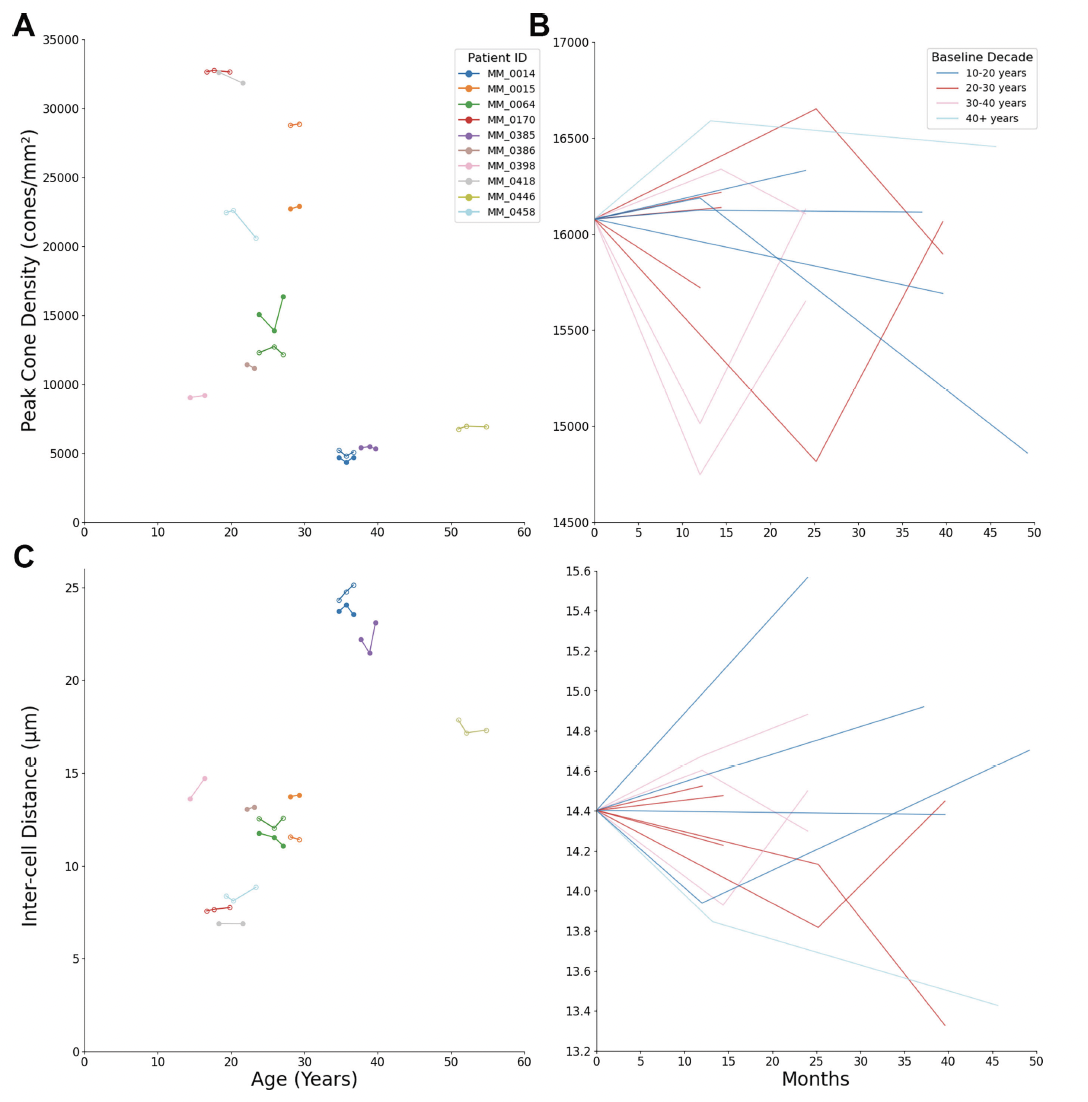
Figure 1. Peak cone density (PCD) and inter-cell distance (ICD) of each eye over the follow-up period. (A, C) PCD and ICD by age, (B, D) PCD and ICD by months of follow-up normalized to the mean baseline of 16,079 cones/mm2 for PCD and 14.4 μm for ICD, and color coded by age at baseline. The younger patients showed greater decline in PCD. OD = solid circles, OS = open circles. This data is licensed under a Creative Commons Attribution 4.0 International License cited by Katta M, Georgiou M, Singh N, et al. Longitudinal imaging of the foveal cone mosaic in CNGA3-associated achromatopsia. Invest Ophthalmol Vis Sci. 2024;65(12):6. https://doi.org/10.1167/iovs.65.12.6
From their results of novel work, the researchers commented that, “this is the first longitudinal assessment of CNGA3-ACHM retinas showing stable foveal cone mosaics over time. The stability of PCD within patients over the follow-up period and the large variability within the cohort means an age cutoff recommendation for potential therapies is difficult to determine. The details of how AOSLO imaging will be used for trial end points or predictive factors in interventional research is yet to be fully elucidated as it has only recently started to be used in clinical trials”.