An international consortium of researchers on a multi-centre study on congenital stationary night blindness (CSNB), led by Oregon Health and Science University Casey Eye Institute, Portland, Oregon, has reported results on genotypes and myopic predictions of a cohort of CSNB patients. The results suggest that myopia in patients with CSNB progresses over time and that the progression is similar among disease caused by genetic variants of CACNA1F, NYX and TRPM1[*], genetic variants situated on chromosome Xp11.23, Xp11.4 and chromosome 15q13, respectively. Researchers suggest that results of their study may “benefit in the future from myopia slowing treatment and practitioners should consider CSNB as a possible diagnosis in early-onset high myopia”.
[*CACNA1F gene: calcium voltage-gated channel subunit alpha1 F, chromosome Xp11.23; NYX gene: Nyctalopin chromosome Xp11.4; TRPM1 gene: transient receptor potential cation channel subfamily M member 1, chromosome 15q13.3; see Gene Cards (https://www.genecards.org/)].
CSNB is a group of inherited retinal disorders (IRD) caused by reduced signaling processing from the cones and rods to the bipolar cells and RPE. The disorder is a clinically and genetically heterogeneous pathology, whereby patients may experience night or dim light vision disturbance, including delayed dark adaptation, and several ocular symptoms on poor visual acuity, myopia, nystagmus and fundus abnormalities. CSNB can be inherited in an autosomal dominant (AD), an autosomal recessive (AR), or an X-linked (XL) disease, and there are at least 17 genes associated to CSNB in the literature. The researchers also stated that, “CSNB is typically associated with high myopia and although several prior case series have described the refractive error of individuals with CSNB, there is a paucity of data on the natural history, axial length, severity, variability and progression of myopia in patients”.
In their study, a multinational, multi-centre, retrospective, longitudinal study was used to evaluate the progression of refractive error in patients with CSNB including sub-group
comparisons of patients with different CSNB genotypes. Seventy-eight (78) patients were included in this study, 41 patients had pathogenic variants in CACNA1F, 22 patients had pathogenic variants in NYX and 15 patients had pathogenic variants in TRPM1. Of the 78 subjects, 69 were myopic at the first visit. The mean (SD) age for the youngest visits were 3.82 (2.73), 3.15 (2.41) and 2.91 (3.16) years for CACNA1F, NYX and TRPM1, respectively. All genotypes showed a significant myopic predicted spherical equivalent of refraction (SER) at birth (-3.076D, -5.511D and -5.386D) for CACNA1F, NYX and TRPM1 respectively and, significant progression of myopia per year (-0.254D, -0.257D and -0.326D) was observed for all three genotypes CACNA1F, NYX and TRPM1, respectively.
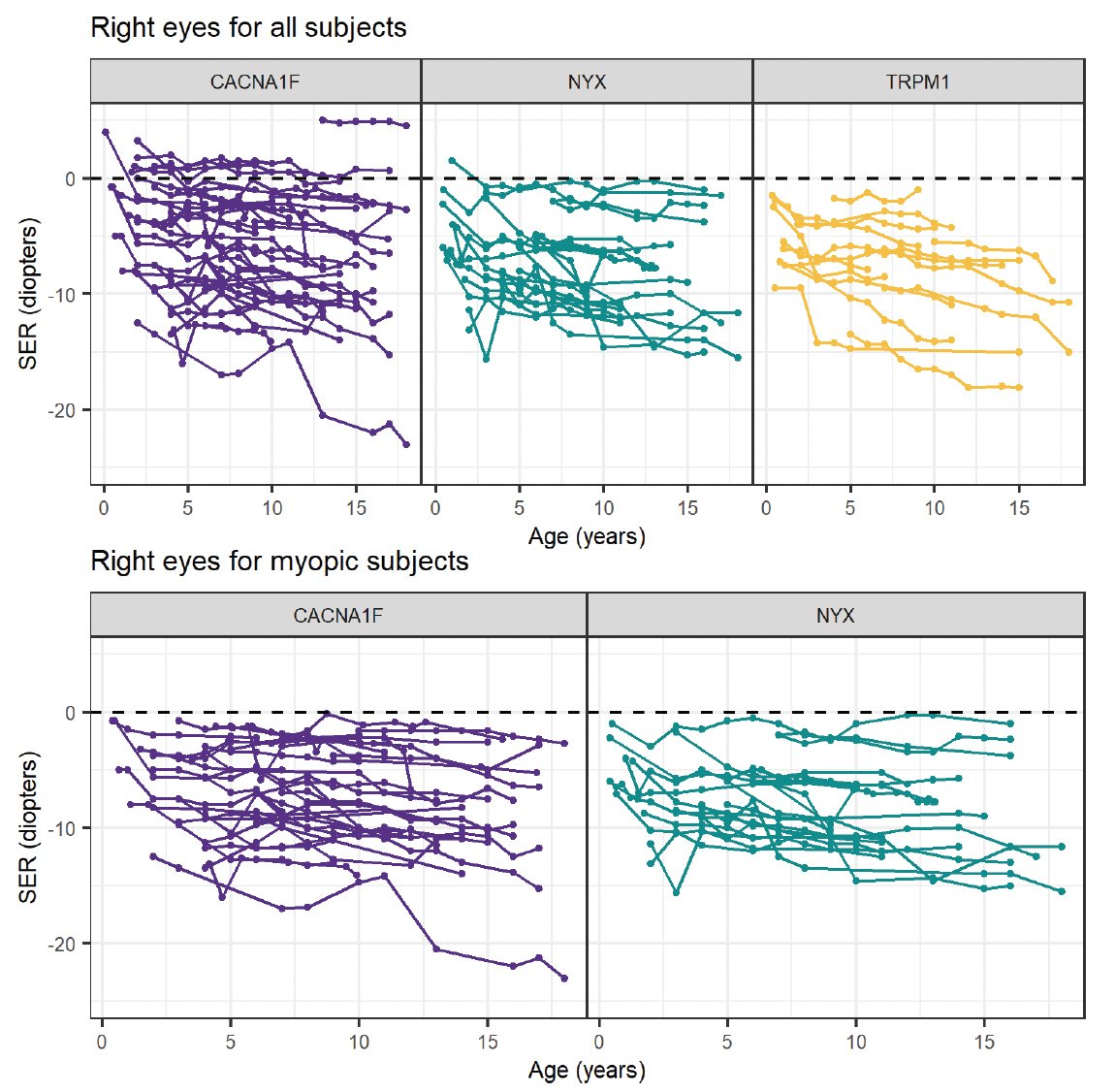
Figure 1: Spaghetti plot showing the trend of SER in patients with variants in CACNA1F, NYX and TRPM1. Each line represents the right eye of one patient overtime. Bottom panels represent patients who began as myopic and had variants in CACNA1F and NYX. SER, spherical equivalent of refraction. (This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/ 4.0/; Igelman et al., Characterising the refractive error in paediatric patients with congenital stationary night blindness: a multicentre study; Br J Ophthalmol 2024;0:1–7).
In summary, the researchers concluded that, “patients with CSNB tend to be myopic from an early age and progress to become more myopic with age”. In particular, the study suggested that patients may benefit from long-term myopia slowing treatment in the future. In terms of managing treatment, the researchers commented that, “overall, these data suggest a moderate to high myopia phenotype that progresses throughout childhood and early adolescence, making CSNB an ideal candidate for an early treatment trial into the efficacy of the use of low-dose atropine in slowing myopia progression in IRDs and thereby reducing further vision loss. In addition, CSNB should always be considered as a potential cause of early-onset myopia. We developed a model that increases our understanding of the natural history of refractive error progression in individuals with CSNB”.